Endangered species: Malnutrition stalks India’s children
How and why are our young ones falling prey to this silent epidemic called acute malnutrition?
• 8.82 lakh Indian children under the age of five died due to malnutrition in 2018.
• We rank 102 out of 117 in the Global Hunger Index 2019, which reported that around 90 per cent of children aged between six and 23 months in the country don’t even get the minimum required food.
• According to the National Family Health Survey 2015-16 (NFHS-4), the Infant Mortality Rate in urban India is 29 as compared to rural which is at 46 per 1000 live births, while the under-five child mortality rate is 34 in cities and 56 in villages.
Stunting (low height for age) is prevalent among 38 per cent of our under-fives and the rate of wasting (low weight for height) of 20.8 percent among our under-fives is the highest in the world.
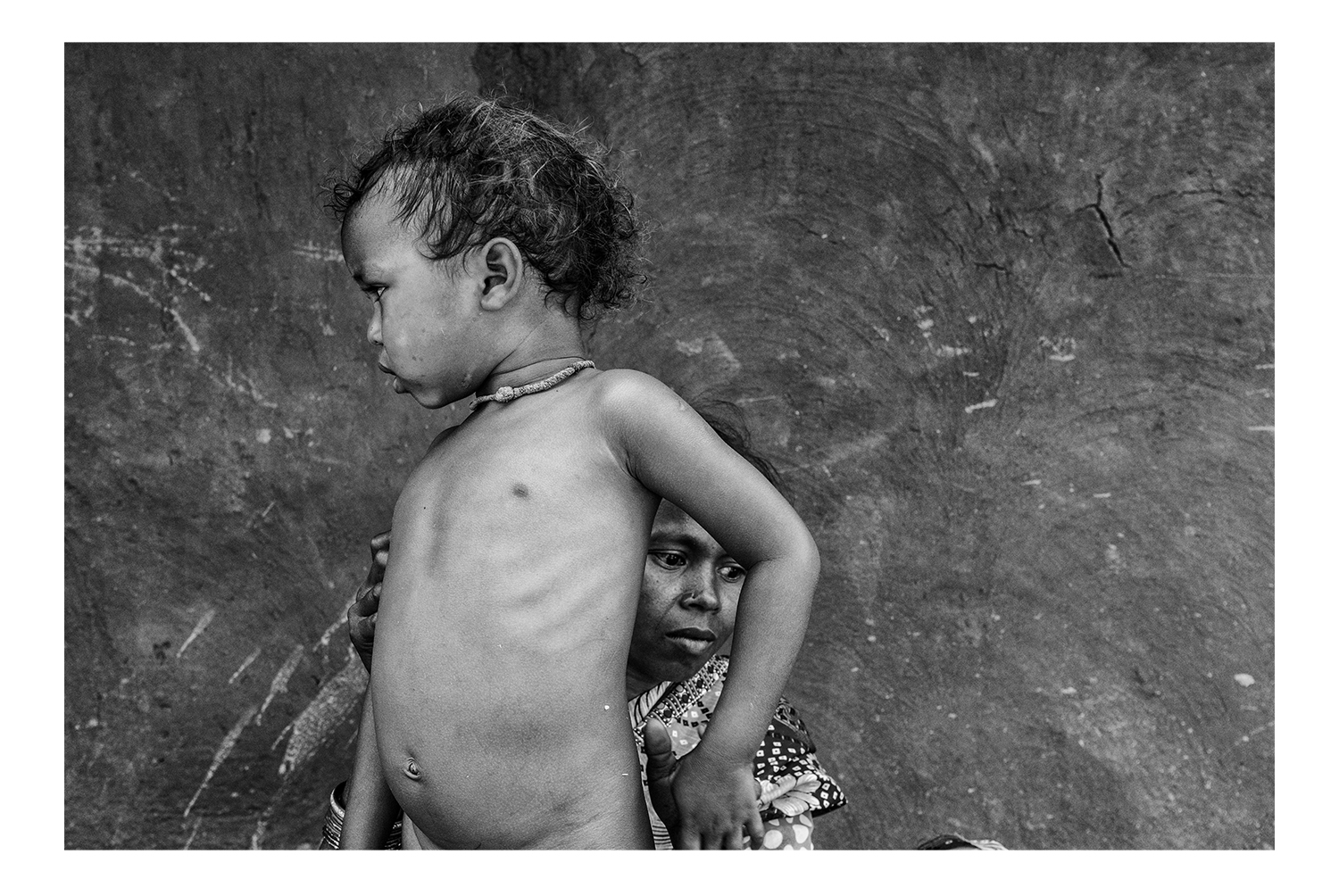
Reed-thin arms, the swelling of oedema distorting their body, some with distended tummies, others wheezing with pneumonia, and most of them with disinterest in their eyes and lethargy in their limbs... this is the state of India’s children. While they may not all be dying of starvation before our very eyes, millions of India’s children are at risk of having lifelong problems because their daily diet does not support their physical and cognitive development. And this is just the tip of the iceberg, as studies estimate that the situation will only escalate further in the years to come.

Many organisations are working to address this huge problem besetting our next generation and its dire repercussions on productivity, but is help reaching the right people? What exactly lies at the end of the chain? How do the Integrated Child Development Services’ (ICDS) outreach programmes via Anganwadi Centres actually work? Are there any success stories that throw light on how things can be done right? It’s only by investigating conditions at the grassroots level that one can get answers that present the true and whole picture.

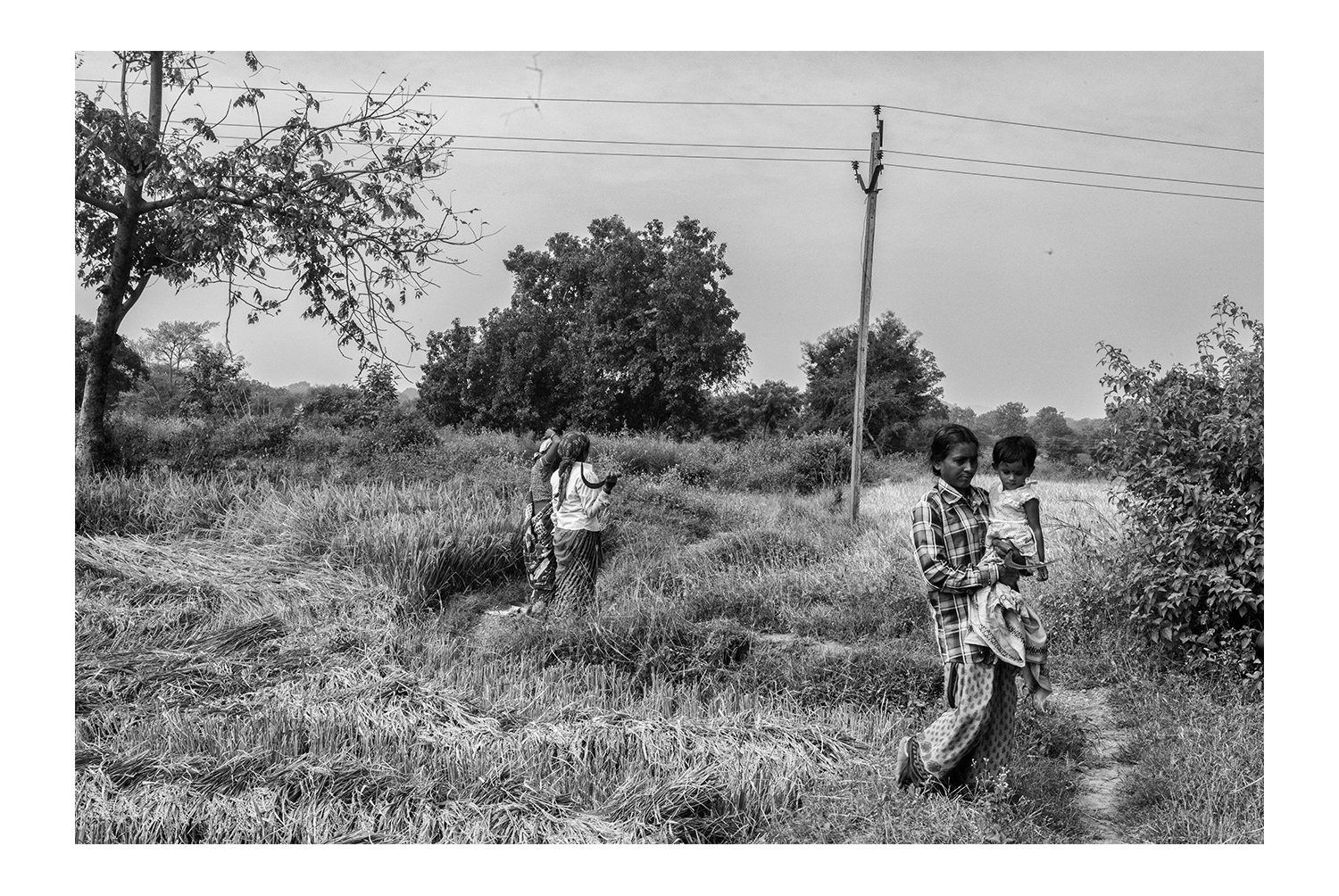
Assam: The gateway to the North East is rich in tea, silk and oil, and receives more rainfall than most parts of India. Despite this, many parts of the state are still grossly under-developed. A high number of people are marginalised and subsist below the poverty line, solely dependent on food entitlements. The vulnerable groups comprise Tea Garden Labourers (TGL), Bodo and Rabha tribes living in areas like the Bodoland Territorial Area Districts, migrant populations of the Brahmaputra floodplains, as well as predominantly Muslim communities in Darrang’s Kharupetia region. Assam continues to be one of the bottom-five states of the country when it comes to health and hygiene. There is a high prevalence of under-nutrition among children, adolescent girls and mothers. The Infant Mortality Rate is high at 48 and 38 percent of children under five years are stunted, primarily due to poor infant and child feeding practices, and poor hygiene and sanitation. Fourteen percent of children suffer from acute malnutrition, with four per cent falling in the category of Severe Acute Malnutrition (SAM).

Chhattisgarh: It is one of the richest states in terms of minerals, even ranking first in coal production. Although rich in history, culture and natural beauty, its population is one of the country’s poorest. A large number of the state’s inhabitants are indigenous tribal groups that often have nutrition-poor food habits, low literacy and subsistence-level economies. Besides, Naxals, armed left-wing extremists, are active in many of the densely-forested districts of this state. According to NHFS-4, the population of Chhattisgarh has high levels of wasting (15 percent),whereas a report by NITI Aayog shows that an alarming 37.6 percent of children below five years in Chhattisgarh are suffering from malnutrition and 41.5 percent of daughters and mothers in the state are anaemic. Home visits in regions high in SAM children such as Dongargaon and other areas surrounding Rajnandgaon, and in the Manpur, Narayanpur and Kanker region gave unique insights into the issue.

Jharkhand: possesses 40 per cent of the mineral resources of India, and is rich in everything from iron ore and coal to uranium, gold and silver. It has been registering a higher rate of economic growth, when compared with the rest of the country, but conversely, reports show that more than 40 per cent of the population lives below the poverty line, about 45 per cent of children under the age of five are stunted, and almost 48 per cent are underweight. Tribals such as Hos and Santals make up a large part of the poorest groups in areas surrounding Chakradharpur.

Maharashtra: It’s considered India’s wealthiest and most industrialised state and is the largest contributor to the country’s GDP (15 percent) thanks to the presence of the financial capital – Mumbai. And yet, Maharashtra also has vast areas where people suffer from scarcity of basic nutrients. Less than a 100 kms from Mumbai, Palghar district has become the epicentre of a SAM crisis over the last two decades. In 2015-2016, there were 555 SAM-related deaths, while the following year saw 475 similar deaths of children. In districts such as Nandurbar and Amravati too, the situation is dire. According to a state government missive, there were almost 94,000 children suffering from SAM in 2018, even though they assert infant mortality has been reduced by 60 per cent from 45 in 2003 to 19 in 2018. While the NFHS-4 reported that the prevalence of SAM in Maharashtra was 9.4 per cent, independent assessments by NGOs suggests that it the actual number could be considerably higher. The population of affected areas is largely tribal communities like Warli, MahadevKoli, Katkari and Thaker.

Odisha: The state has a wealth of history, agriculture, forest resources, gemstone, bauxite, folk dance, folk music, folklore and handicrafts. But, with 9.59 million-strong tribals making up almost 23 per cent of Odisha’s total population, and 13 of the 62 tribal communities belonging to Particularly Vulnerable Tribal Groups (PVTGs), certain pockets of the state show an alarming rate of malnutrition. As per UNICEF data, about 57 per cent of tribal children in the under-five year segment are chronically undernourished and infant mortality among tribal communities in Odisha is 92, higher than in the rest of the country. As many as 26,184 children suffered from malnutrition and fell in the severely underweight category in 2018. State Women and Child Development (SWCD) department data shows that the number of children suffering from malnutrition is the highest in the districts of Kalahandi (3,114), followed by Kandhamal (2,887) in 2018. Nearly 3,500 children have died of malnutrition here during the last five years. In fact, Kalahandi has been associated with backwardness and starvation death since the 1980s, giving rise to the term ‘Kalahandi Syndrome’. The India Health of Nation and States 2017 report cited malnutrition among children and mothers, as the top reason for death and disability in the state.
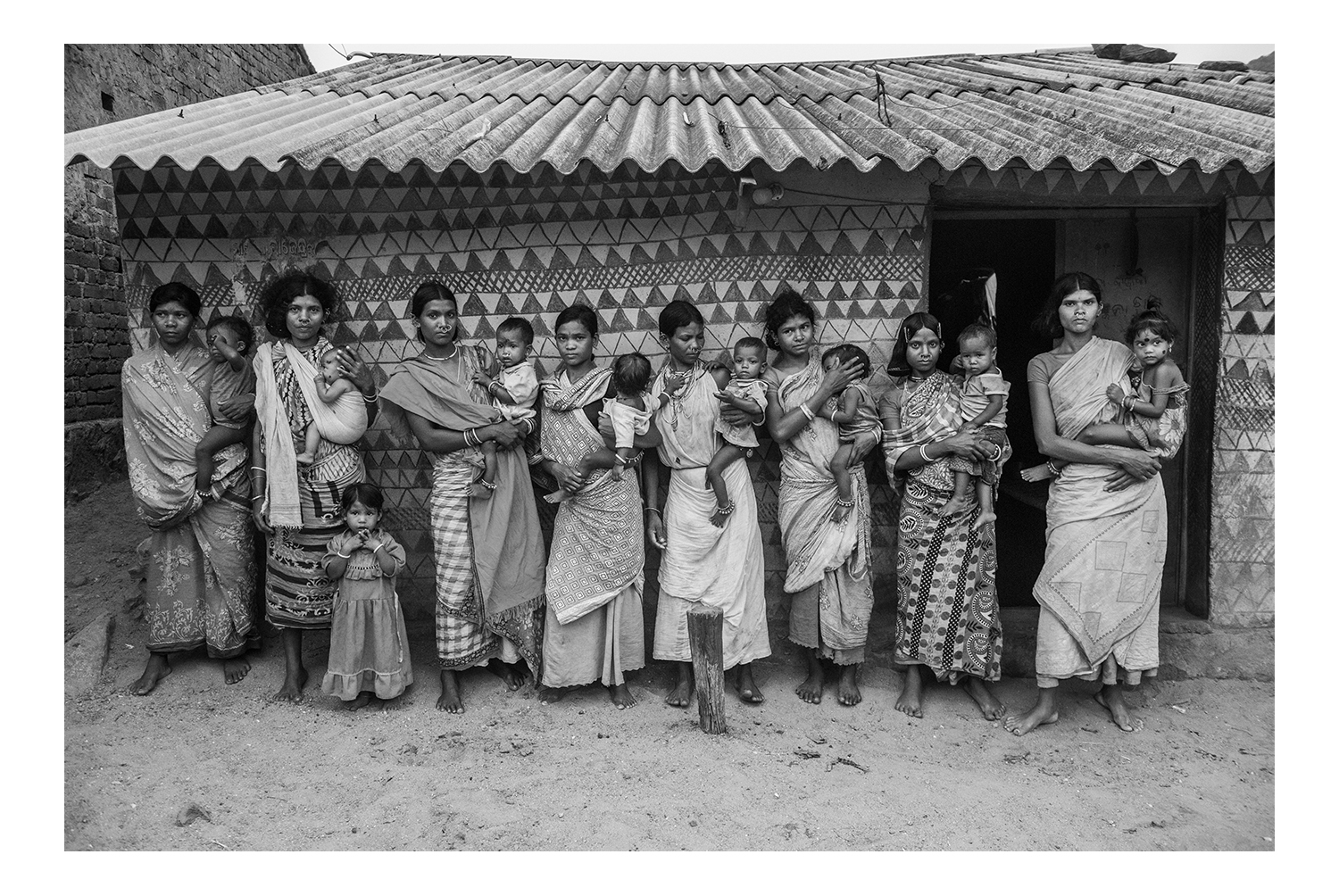
Not surprisingly, we found that the incidences of stunting, wasting and malnourishment were high in these populations, with an inordinately large number of children falling in the Severe Acute Malnutrition (SAM) category, which is the most extreme and visible form of undernutrition. We talked to the families of these children; we visited the district nutrition rehabilitation centres; we watched the women who have made it their life’s work to bring about change as they went about their daily duties... just to understand where it’s all going wrong. We found that, apart from poverty, which is the most obvious, many other factors contribute to dismal conditions in the homes of the tribal community and other marginalised sections of society. Unavailability of education, hygiene and access to medical treatment, early marriage, multiple pregnancies, lack of nutrition from earlier generations, superstitious beliefs and faith in dubious medicine men instead of doctors, and many other reasons compounded the problem. The sheer lack of awareness amongst parents about what constitutes a nutritious meal was one of the most startling findings. In many cases, the failure of the system to provide aid to the beneficiaries as well as to people who are working in the field also added an extra pall of gloom to already dire realities - PRIYA PATHIYAN 2019.
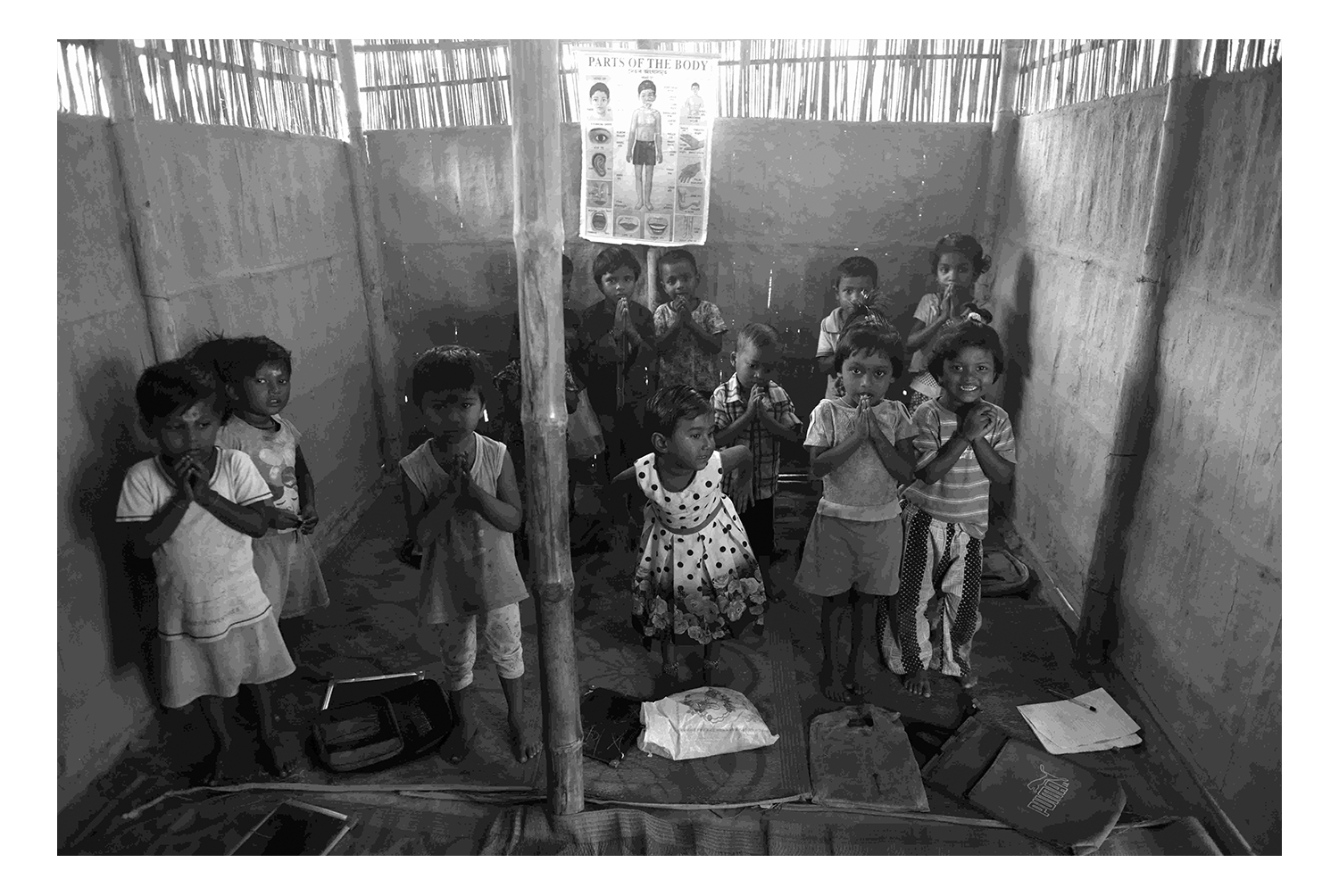
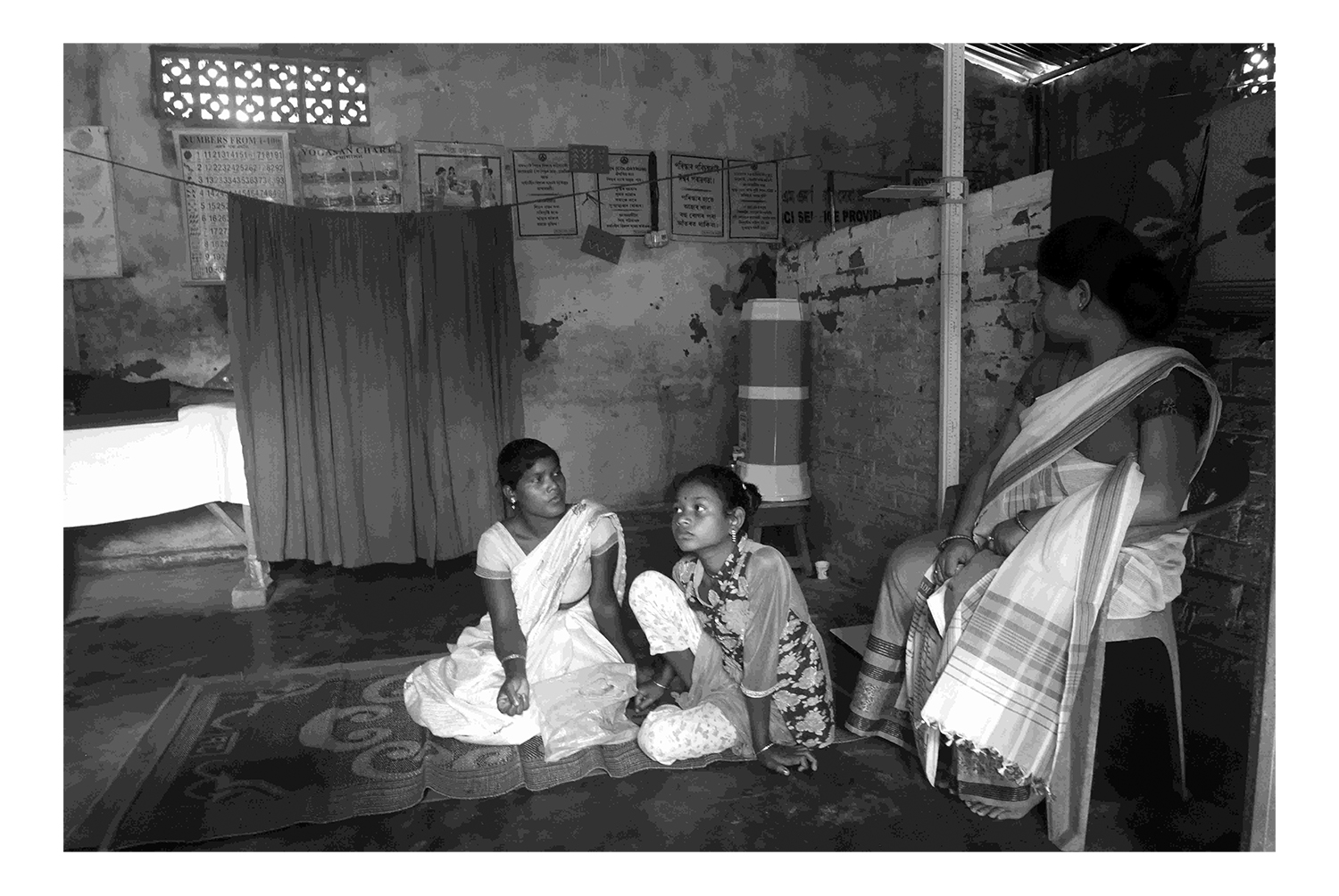
Anganwadis: Rural lifelines
An airy room with plenty of floor space, scrupulously scrubbed clean. Everything from windows and doors to utensils neatly labelled. A row of identical bags with a child’s name tacked on each one hanging across a wall. In an adjoining room, a lady cooks a hot meal for the children and mothers expected to arrive any minute. This is the typical scene every morning in almost 1.4 million Anganwadis across India. These rural childcare centres were first introduced as far back as 1975 as part of the Integrated Child Development Services programme to combat child hunger and malnutrition. These centres provide supplementary nutrition, non-formal pre-school education, nutrition and health education and counselling, immunisation, health check-ups and referral services in conjunction with public health systems. The Anganwadi workers make regular home visits in surrounding villages, keeping meticulous records of the health of adolescent girls, expectant mothers and children. They spot those who need facility-based care and recommend admission to the district’s Nutrition Rehabilitation Centres. In most areas where food is scarce, the villagers depend on the mid-day meal served at the Anganwadi. The community-based network has great potential for creating change. Already, a few states have started to digitise the voluminous records and others plan to follow suit by introducing the ICDS-CAS scheme, which will involve training the Anganwadi Workers to input data into an integrated system via their mobile phones.





Customs and rituals
India’s rootedness in its culture may help to give us a sense of deep belonging. But it is also associated with many archaic traditions that are detrimental to many members of society. Women, though worshipped as powerful goddesses, do not enjoy such a status in the flesh. Often victims of violence and patriarchy, they seldom have a voice in their households and are often treated like second-rate citizens. Although the menstrual cycle is part of the process of reproduction, it is considered unclean and women going through the discomfort are made to further suffer the ignominy and inconvenience of being segregated from the family during these days. In some areas, a new mother is kept isolated for up to a month after birthing her baby. Their general suspicion of institutional healthcare sees tribals and other villagers frequenting medicine men whose repertoire includes chants, talismans and dubious concoctions. This results in wastage of time and them approaching hospitals only as a last resort, by which time the situation is already beyond repair. It is necessary to change these medieval mindsets through education and awareness for the progress of society as a whole.





The negative impact of culture and circumstance
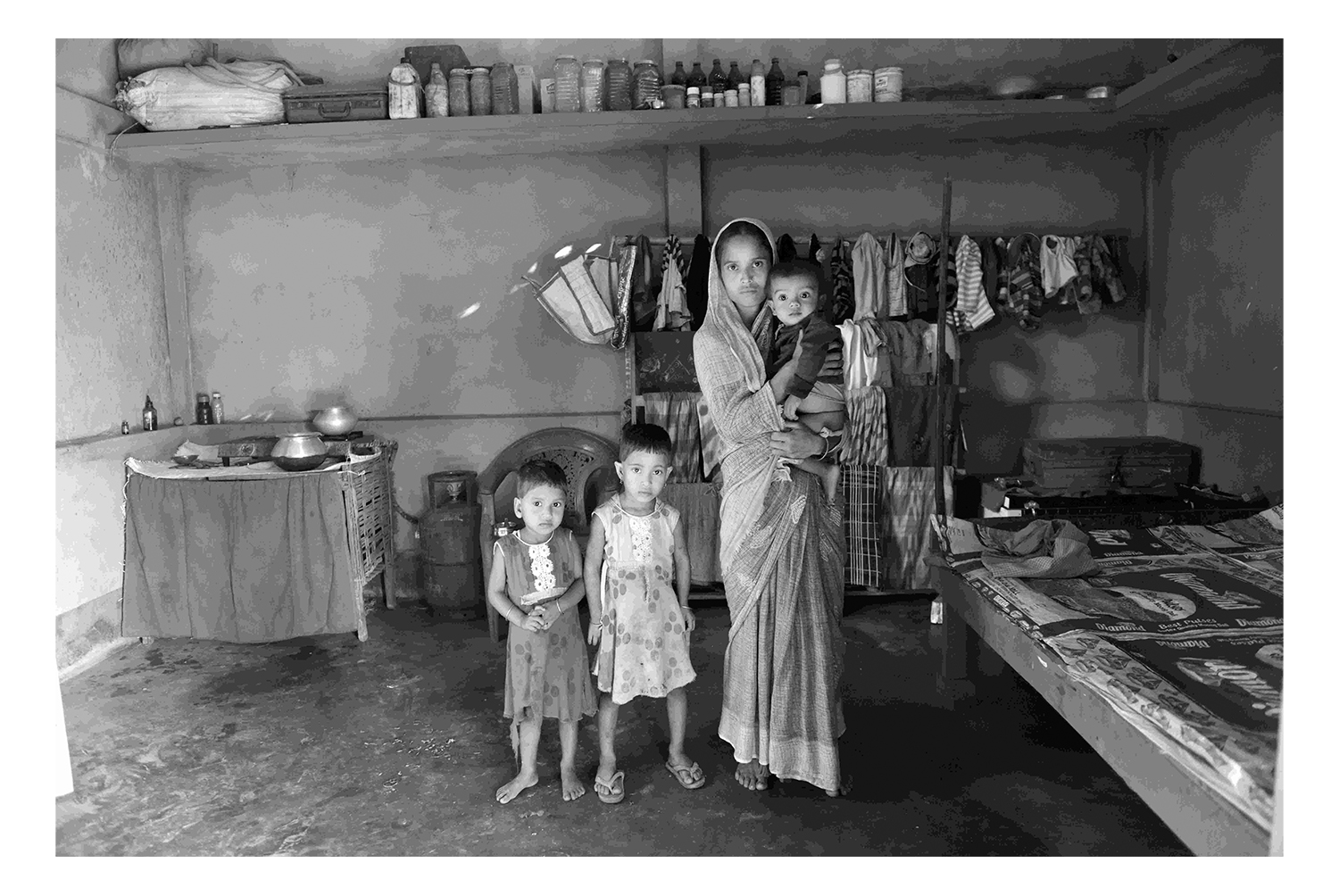
In Assam’s Darrang district, there is a Muslim majority in the outlying areas of Kharupetia town. This population, though literate, is beset by a number of issues such as early/multiple marriages, violence against women, lack of birth control and spacing between children, extreme poverty and, in some villages, a failure on the part of the government to provide food supplies.
The morose mood extends to the Anganwadi nearby. Mukhida Begum is with her son Murshidul Islam (3) weighing only eight kilos, in the hope of getting him one square meal. Mujahidul Islam (almost 3) is with his grandmother HanufaKhatoun. This SAM child is suffering pneumonia and a low weight of 9.3 kilos. His mother died in a fire just a month after giving birth and his frail grandmother has looked after him ever since. ShahnazParveen (12 months) weighs only five kgs 900 grams now even though she was born three kilos, as her mother Nazma has to work in the fields all day and cannot breastfeed her. Aakhirul Ali (seven months) had a birthweight of only 2.5 kilos, which has since only increased to 5.5 kilos. His mother Rabiya Begum says she is unable to breastfeed and he survives on rice, biscuits or cake, whenever he gets them. Siblings AashiqTaluqdar (4) and Afrida (34 months) are with their mother Murshida Begum. Aashiq weighs only 11 kilos, while his sister has a normal weight of 12 kilos. Their parents Murshida and Noor Islam are at a loss to explain why there is such a vast difference between the two.





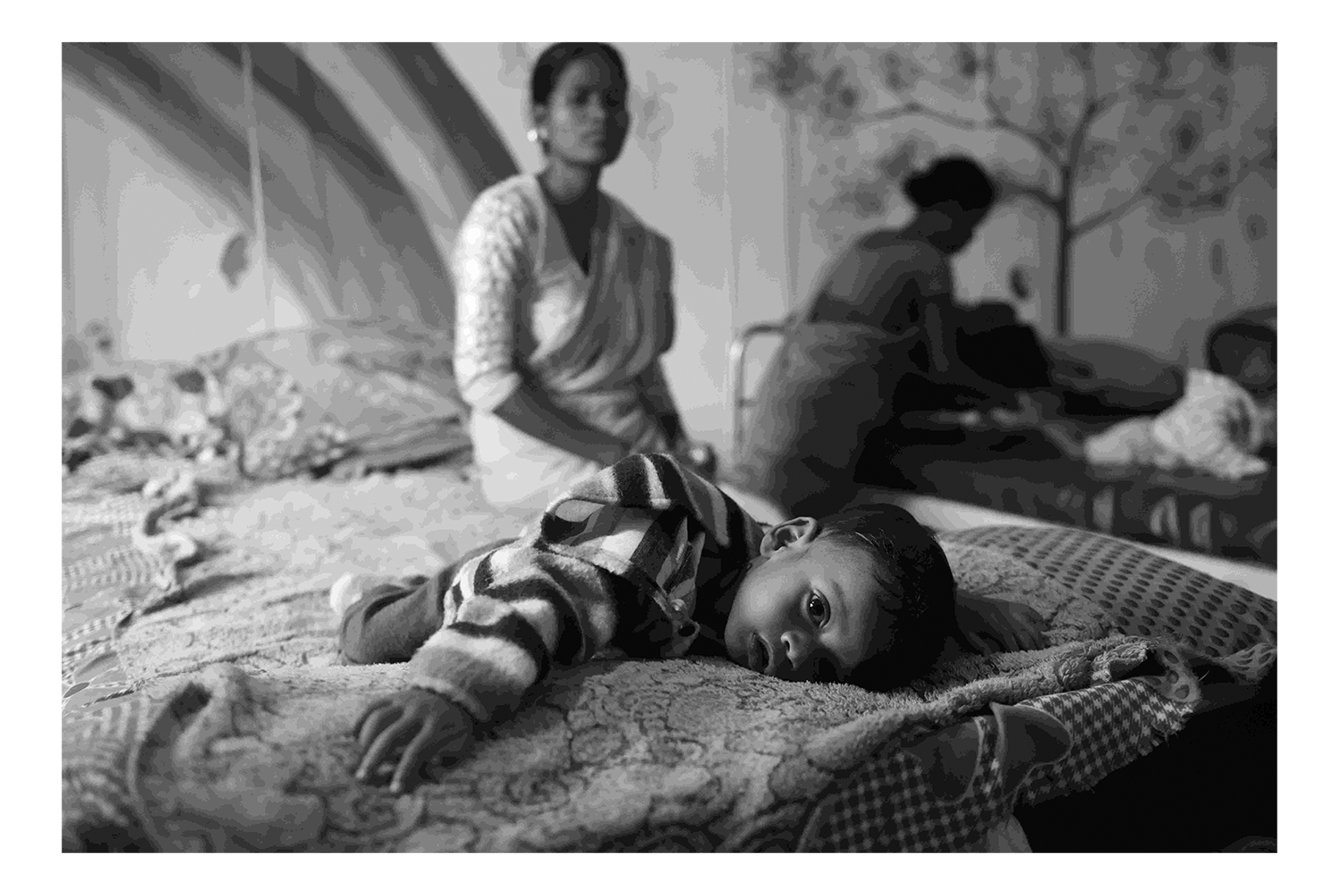
The crucial role of the Nutritional Rehabilitation Centres
The Ministry of Health and Family Welfare has established 1151 Nutritional Rehabilitation Centres (NRCs) across the country under the National Health Mission. They provide facility-based care for children with Severe Acute Malnutrition (SAM) and medical complications. As per the National Family Health Survey (NFHS 4, 2015-16), 7.5 per cent of under-fives are severely wasted and 35.8 per cent of children are underweight. Children with Severe Acute Malnutrition (SAM) along with medical complications are referred from villages by frontline workers such ASHA and Anganwadi ladies, who make home visits, and admitted to NRCs as per the defined admission criteria. These NRCs offer appropriate feeding of children, careful height and weight monitoring, and counselling to mothers and caregivers on age-appropriate caring, nutrition and growth monitoring. Nutritionists that we met in NRCs were passionate about their work and used many innovations to explain the importance of a balanced diet for the children to their mothers. Sadly, as there aren’t enough of these centres and usually just about 10-12 beds in each, sometimes there is a long wait, which discourages parents. NRC functionality differs from area to area, depending on the quality of training imparted to the staff, equipment provided, etc. According to reports, 1.86 lakh under-five children were admitted in the NRCs in the year of 2017-18, of which 1.17 lakh children were discharged with target weight gain, so there is hope for success along with scope for improvement.








The Caste Factor
Although negative discrimination on the basis of caste has been forbidden by the Indian Constitution for almost seven decades, it is still one of the most prevalent social evils in our country. While those in its upper echelons often don’t realise the privilege it automatically confers on them, it’s the people at the lower end of the caste spectrum that bear the brunt of it every day and in every possible way even in the 21st century. Although there are educational, professional and political reservations for members belonging to Scheduled Castes and Scheduled Tribes, a large proportion of those who live in remote rural areas are completely cut off from these reformative measures that seek to undo the centuries of prejudice and inequality. Their reality hasn’t changed and they are firmly ensconced in the traditional roles their clans have served since time immemorial. And while men from the lowest castes may suffer, it’s the women that suffer the most, receiving the least amount of medical attention and nutrition.
It’s the harvest season and the entire village of Chawad in Chhattisgarh is hard at work in the fields or carrying bundles to their storage rooms. Satrupa and PremlalSahu take turns to work in their family’s fields while the other looks after their two children. Tushar (9) is active though he is underweight. And their toddler Lokprabha (18 months), who was only two kilos when she was born, is now just 8.5 kilos. The worried parents have taken her into Dhamtari town for check-ups. The doctors tell them there’s nothing wrong but they are tense as her weight doesn’t go up whatever they do.



The reality behind tea
Tea Garden Labourers (TGL) make up about 20 percent of the population of Assam, which produces more than half of India’s tea. The ancestors of the current TGLs were tribals and backward castes brought in from neighbouring states and forced to work on the British plantations as indentured labourers from the mid-nineteenth century to the mid-twentieth century. At that time, they were little more than slaves, with no rights, no freedom and minimal access to medicines or education. Even today, they are among the most exploited and under-developed communities in the state. Reports estimate the TGL population to be around 6.5 million, a large number of which still lives in quarters provided by the 800-odd tea estates across Assam. These workers earn just about Rs 167 per day, with a few benefits and accommodation. They are not integrated into the Assamese populace, as the high-caste Hindus look down upon them as interlopers. The women are especially at the lowest end of the chain. Many of them have to cope with violence in the home from husbands addicted to country liquor, work through their pregnancies, return to work soon after childbirth thus denying their babies proper nutrition through exclusive breastfeeding, and also have to face sexual harassment from plantation managers and other authority figures. Some of them who don’t have extended family, are forced to take their babies to the tea plantation as they have no access to daycare facilities. Although they make up the largest female workforce in the country, they don’t have representation that empowers them to bring about change.





